

Walking isn’t enough. Not after 50.
That might sound blunt, but the research is clear. Walking produces ground reaction forces of roughly 1.2 times your bodyweight. Maintaining bone density after menopause requires forces exceeding 4 times bodyweight — the kind generated by squats, lunges, deadlifts, and impact training. Walking doesn’t come close.
And bone isn’t the only thing at stake. After age 30, women lose 3–8% of their muscle mass per decade. After 50, that rate accelerates to 5–10% per decade. After 60, it jumps to roughly 3% per year. The drop in estrogen during menopause makes all of this worse — accelerating sarcopenia, increasing visceral fat, reducing insulin sensitivity, and raising cardiovascular risk.
High-intensity exercise — both HIIT and heavy resistance training — directly counters every one of those changes.
- What happens to a woman's body after 50
- Why high-intensity training specifically
- The three types of high-intensity exercise aging women need
- What if you've never done high-intensity exercise before
- Joint-friendly alternatives that still deliver intensity
- How often and how long
- Safety first — always
- Frequently asked questions
What happens to a woman’s body after 50
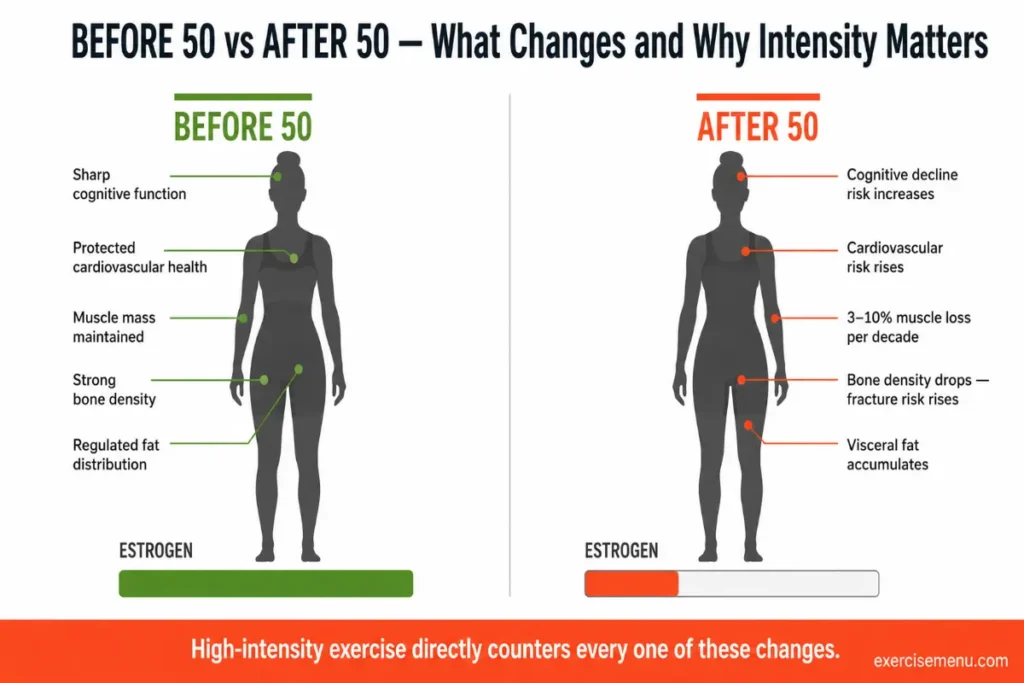
Menopause is the inflection point. Estrogen does more than regulate your cycle — it helps your body hold onto muscle, keep bones dense, manage where fat is stored, and protect your heart. When estrogen declines during perimenopause and drops further post-menopause, the body loses those protections simultaneously.
The consequences stack up. Muscle mass drops — by as much as 15% in the years following menopause. Bone mineral density falls, increasing fracture risk. Fat accumulates around the abdomen, driving insulin resistance and raising the risk of type 2 diabetes and cardiovascular disease. VO2 max — your body’s capacity to use oxygen during exercise — declines steadily, reducing stamina and energy.
None of this is inevitable. Every single one of these changes responds to the right kind of training.
Why high-intensity training specifically
Low-to-moderate exercise helps. It reduces stress, improves mood, supports heart health. Nobody is arguing against a daily walk. But for the specific changes that menopause triggers — bone loss, muscle wasting, metabolic slowdown, fast-twitch fiber atrophy — the stimulus needs to be stronger than moderate.
Here’s why. Your body preferentially loses fast-twitch muscle fibers as it ages. These are the fibers responsible for explosive power, strength, and the ability to catch yourself when you trip. Walking and light cardio don’t recruit them. Only high-force movements — heavy resistance training, sprinting, jumping, HIIT — activate fast-twitch fibers enough to prevent their decline.
A study from the Mayo Clinic found that HIIT-style training increased mitochondrial health in older participants more than any other exercise form. The decline in cellular energy production that comes with aging was essentially reversed with intense exercise. The effect was most pronounced in the older group — not the younger one.
Professor Debra Anderson and Dr. Charlotte Seib, writing in the journal Maturitas, reviewed five years of evidence on exercise and aging women over 50. Their conclusion: women who exercised at higher intensities — what they described as “huffing and puffing levels” — for 30–45 minutes per day, at least five days per week, significantly reduced their rate of death and disability while reporting better physical function than those who stuck to moderate activity.
The three types of high-intensity exercise aging women need
Not all high-intensity exercise is the same. The most effective approach combines three types — each targeting a different system that declines with age.
1. Heavy resistance training
This is the non-negotiable. The NSCA specifically recommends higher-intensity lifting for adults over 50 — 2–3 sets of 1–2 multi-joint exercises per major muscle group at 70–85% of your one-rep max. Compound movements — squats, deadlifts, rows, overhead presses, lunges — form the foundation because they load multiple joints and large muscle groups simultaneously. The key is applying progressive overload — gradually increasing the weight or reps over time so the stimulus keeps driving adaptation.
An 8-week study by Hoier et al. (2021) at the University of Copenhagen put post-menopausal women (mean age 64, more than 10 years past menopause) through supervised high-intensity cycle training three times per week. Results: 18% increase in VO2 max, 4.9% reduction in fat mass, improved HDL cholesterol, and measurable improvements in blood vessel function and metabolism at the cellular level.
Heavy resistance training also tells your body to build more bone while slowing down the process that breaks it down. A 2025 review published in Current Osteoporosis Reports confirmed that supervised high-intensity resistance and impact training (HiRIT) is effective at increasing lumbar spine bone mineral density and is safe and well-tolerated in post-menopausal women with osteoporosis.
2. HIIT (high-intensity interval training)
HIIT alternates short bursts of all-out effort with recovery periods. The structure can be adapted to nearly any activity — cycling, rowing, swimming, stair climbing, even walking intervals for those just starting.
What makes HIIT particularly valuable after menopause is its effect on metabolism and body composition. A 2025 meta-analysis in Frontiers in Aging found that HIIT significantly improved body composition, insulin resistance, blood lipids, cardiorespiratory fitness, sleep quality, and anabolic hormone levels in elderly women — outperforming moderate-intensity continuous training across nearly every measure.
HIIT sessions don’t need to be long. Five to ten minutes of genuine high-intensity work produces measurable improvements in executive function, brain blood flow, and BDNF levels — a protein linked to cognitive health and dementia risk reduction.
3. Impact and balance training
Falls are the leading cause of injury-related death in older adults. Balance training reduces fall risk directly. Impact training — controlled jumping, stepping, and landing — builds the bone density that prevents fractures when falls do happen.
A practical approach: include 2–3 balance exercises (single-leg stands, heel-to-toe walking, lateral step-overs) at the end of each resistance session. Add low-impact jumps or step-ups once your strength base supports them safely.
What if you’ve never done high-intensity exercise before
This is where most programs lose people. The jump from “I walk three times a week” to “squat at 80% of your max” is too large. The bridge matters more than the destination.
Weeks 1–2: Brisk walking intervals — 2 minutes fast, 2 minutes easy. Repeat for 20 minutes. Add 2 sets of 10 bodyweight squats and 2 sets of wall push-ups on alternate days.
Weeks 3–4: Replace 2 walking sessions with cycling or rowing intervals — 30 seconds hard, 60 seconds easy, for 10 minutes total. Continue bodyweight strength work, adding lunges and glute bridges.
Weeks 5–6: Introduce light dumbbells or resistance bands to your strength exercises. Reduce rest between HIIT intervals to 45 seconds. Increase strength work to 3 sets.
Weeks 7–8: Full HIIT circuit — 20 minutes. Full resistance training — compound movements with progressive overload applied. You’re now training at the intensity your body actually needs.

The key is gradual progression — not jumping straight into box jumps and heavy deadlifts on day one. Every session should feel challenging but manageable. If form breaks, the intensity is too high. Scale back and build again.
Joint-friendly alternatives that still deliver intensity
Not every body can squat heavy or sprint. Arthritis, past injuries, joint replacements — these are real constraints. But intensity doesn’t require impact. These alternatives deliver the stimulus without the joint stress:
Swimming intervals — sprint one lap, recover one lap. Water supports bodyweight while allowing maximal effort.
Cycling HIIT — stationary bike, 20 seconds all-out, 40 seconds easy. Zero joint impact, full cardiovascular and metabolic demand.
Rowing — full-body, low-impact, high-intensity potential. Engages legs, back, arms, and core in every stroke.
Shadow boxing — standing punches and combinations at speed. Elevates heart rate, builds upper body power, requires zero equipment.
Water aerobics at intensity — not the gentle version. Explosive movements against water resistance build strength and cardiovascular capacity while fully supporting joints.
The exercise doesn’t matter as much as the intensity behind it. If you’re not breathing hard, the stimulus isn’t strong enough to drive the changes your body needs.
How often and how long
The CDC recommends 150 minutes of moderate aerobic activity per week or 75 minutes of vigorous activity for adults over 65. For aging women specifically, the evidence supports going beyond that minimum.
A practical weekly structure:
| Day | Session | Duration |
|---|---|---|
| Monday | Resistance training (compound lifts) | 30–40 min |
| Tuesday | HIIT (cycling, rowing, or walking intervals) | 15–20 min |
| Wednesday | Rest or light mobility/stretching | 20 min |
| Thursday | Resistance training (compound lifts) | 30–40 min |
| Friday | HIIT or swimming intervals | 15–20 min |
| Saturday | Balance and flexibility work | 20 min |
| Sunday | Rest | — |
Adjust frequency based on recovery. Two resistance sessions and two HIIT sessions per week is the minimum for meaningful adaptation. Three of each is ideal if recovery supports it. Reps, sets, and intensity for adults over 50 covers the specific programming details.
Safety first — always
Medical clearance before starting. Full stop. If you have a heart condition, uncontrolled blood pressure, severe osteoporosis, or any condition that affects your ability to exercise safely, your doctor needs to know your plan before you begin.
Beyond clearance, three non-negotiable rules: warm up before every session — five minutes of light movement primes your joints and nervous system. Stay hydrated before, during, and after. And if something hurts beyond normal muscle fatigue — sharp pain, joint pain, radiating discomfort — stop. Muscle soreness after a hard session is expected. Joint pain is a warning.
Working with a personal trainer, even for a few initial sessions, reduces injury risk significantly. A trainer who understands menopause-specific needs can modify exercises for your joints, monitor form, and adjust intensity appropriately.
Frequently asked questions
Is HIIT safe for women over 50?
Yes — when progressed gradually and performed with proper form. Harvard Health, the ACSM, and the Mayo Clinic all support high-intensity training for older adults. Start at a lower intensity and build over 4–8 weeks. Medical clearance is recommended before beginning.
Can you build muscle after menopause?
Yes. Post-menopausal women can build muscle with progressive resistance training. Estrogen decline makes it harder but not impossible. The NSCA recommends loads at 70–85% of your one-rep max, 2–3 sessions per week, targeting all major muscle groups with compound movements.
How do I know if I’m exercising at high enough intensity?
The talk test: if you can hold a full conversation, the intensity is moderate. If you can only say a few words between breaths, you’re in the high-intensity zone. If you can sing, pick up the pace.
Will high-intensity exercise make my joints worse?
Not necessarily. Properly loaded resistance training strengthens the muscles, tendons, and ligaments that support joints. If you have arthritis or joint issues, low-impact alternatives — cycling, swimming, rowing — deliver the same metabolic and cardiovascular benefits without the joint stress.
What if I can only walk right now?
Start there. Walking intervals — 2 minutes brisk, 2 minutes easy — are a legitimate entry point to high-intensity training. Over 4–8 weeks, progress to faster intervals, longer durations, and eventually add bodyweight strength work. The 8-week progression plan above bridges the gap from walking to full HIIT.
Does high-intensity exercise help with hot flashes?
Research from the University of Utah suggests that regular high-intensity exercise can reduce the severity and frequency of hot flashes. The effect likely relates to improved thermoregulation and hormonal balance that comes with consistent training.